
Ivermectin/Hydroxychloroquine
All posts tagged Ivermectin/Hydroxychloroquine
It does seem many of our governments are anti-citizen!
Our governments have betrayed the citizens. The following is an email from the united Australia Party.
‘More truth is being exposed about the medical and political response to the Covid-19 pandemic with the Therapeutic Goods Administration (TGA) yesterday removing restrictions on the prescribing of ivermectin.
Long lauded as a safe, effective and inexpensive treatment, ivermectin was seen by many in the medical profession as way through the pandemic that could have helped treat Covid-19 patients and potentially saved countless lives.
In their statement which can be read HERE, the TGA say the ban has been reversed as “there is sufficient evidence that the safety risks to individuals and public health is low when prescribed by a general practitioner in the current health climate”.
Many esteemed medical minds – including Dr Pierre Kory who spoke at the UAP Covid-19 Vaccine Conferences – suggested bans on ivermectin were in place purely for political and financial reasons, given that multiple studies, trials and billions of use cases had proved it to be a safe, effective drug.
The TGA’s latest move all but confirms what many believed to be the truth – that ivermectin was removed from use because it threatened vaccine take-up being much cheaper than the vaccines and in plentiful supply.
In reality, the ban removed a legitimate treatment option for the sick, while the government persisted (and still persist) in pushing an experimental vaccine for the healthy, while all the time refusing to address the vaccine’s dangers or provide a plausible explanation for the shocking rise in excess deaths.
After the TGA’s withdrawal of AstraZeneca as an approved Covid-19 vaccine in late March this year and now the lifting of the ivermectin ban, the TGA are effectively shining a spotlight on themselves, their practices and their public messaging during the pandemic.
The restoration of doctors’ rights to prescribe ivermectin is a win for those such as Clive Palmer and Craig Kelly who spoke out bravely in face of relentless attacks from governments and government agencies, along with the millions on social media who were taken in by the myth that ivermectin was a ‘horse worming drug’ and labelled its advocates as ‘anti-vaxxers’ and ‘cookers’.
As more and more truths are revealed about the lies that were peddled and perpetuated to Australians, along with the role of big pharma and government in the censorship of important safety information that prevented people from making informed decisions, calls for a Royal Commission will surely grow louder.’
Romans 10:13 For whosoever shall call upon the name of the Lord shall be saved.
‘The concealment of vaccine induced deaths by Australian regulators, brought to light in a recent series of conferences presented by the United Australia Party, has sent shockwaves around the country.
United Australia Party Chairman, Clive Palmer, praised the courage of the medical experts who spoke at the sold-out conferences, which were attended by many thousands of concerned Australians in Melbourne, Sydney, the Gold Coast and the Sunshine Coast.
Referring to a current article by one of the key speakers, renowned American cardiologist Dr Peter McCullough, Mr Palmer said the exposure of “wilful concealment” by the TGA should be greatly concerning for all Australians.
Dr McCollough wrote: “In an explosive set of public lectures, crowded halls filled with thousands of Australians learned from Dr Melissa McCann (BPharm, MBBS, FRACGP), who also holds a Graduate Certificate of Allergic Disease, that Dr John Skerritt and the TGA had determined that several previously healthy young children died of COVID-19 vaccine induced myocarditis. Redacted letters from the TGA to Dr McCann indicated these facts and an admission of wilful concealment.
“The dossier included letters of concern from Dr McCann, other doctors and the responses from Skerritt. Alarmingly, Skerritt and the TGA did not want to go public with these cases in order to keep the vaccine campaign going without “vaccine hesitancy” among a weary public who were witnessing countless injuries, disabilities, and deaths with repeated injections.
Dr McCann showed each letter and the causality determination with the vignette of victim after victim.”
Clive Palmer said the huge public response to the Australian vaccine conferences highlighted the public’s concern in the breach of public safety by the TGA.
“I commend those Australians who voted with their feet in attending these conferences and the brave medical experts for sharing their expertise in bringing these important matters into the public domain,” Mr Palmer said.’https://www.unitedaustraliaparty.org.au/conferences-expose-wilful-concealment-of-vaccine-induced-deaths/
‘Dr. Pierre Kory, Chief Medical Officer of the FLCCC, and Dr. Paul Marik, Chief Scientific Officer, recently made updates to I-RECOVER: Post Vaccine Syndrome to address these concerns.
First, it is important to understand that not everyone who gets a COVID-19 vaccine will react in the same way. Dr. Kory describes three distinct groups:
“There are people who come to my practice who are vaccine-injured,” he says, “and they present with a constellation of symptoms.” Dr. Kory uses several strategies to try to help these patients, depending on their main complaints and the severity of their symptoms.
A second category of patients is experiencing a single complication caused by the vaccine rather than a myriad of symptoms. Treatments are also available for these patients and are often quite successful.
“Then you have people who have been vaccinated and are asymptomatic,” Dr. Kory goes on to explain. “They don’t have any acute or chronic symptoms.” These are often the people who are most concerned about whether they have a potential ‘ticking time bomb’.
The four- to six-month window
For these people, there is some good news depending on the date of their last injection. If your last vaccination or booster was more than five or six months ago and you’ve experienced no adverse symptoms, you are likely in the clear.
“We used to say most people who are vaccine injured have symptoms within days to weeks,” says Dr. Marik, “so if you’re beyond that we used to say you’ve dodged a bullet and you’re OK. But it seems like there are people who are otherwise healthy, who have no signs and symptoms of vaccine injury, and who within this window of four to six months die suddenly from an acute cardiac event.”
There are two peak windows when deaths that may be linked to vaccination seem to occur. “They happen either within a few days, which we think is acute heart inflammation causing myocarditis and then a fatal arrhythmia,” says Dr. Kory. “And then there are those that die around five months later.”
“If you are well after five months out, or a year out, with no symptoms, no problems, I really do want to reassure you that I think you’re okay.”
Dr. Kory and Dr. Marik, along with other colleagues of theirs, think the deaths that happen around the five-month peak are related to massive fibrin clots.
“If you are well after five months out, or a year out, with no symptoms, no problems, I really do want to reassure you that I think you’re okay,” Dr. Kory says, noting that many people have had no reaction to the vaccines.
If you were vaccinated or boosted within the past five months and are now worried because of the emerging evidence and data showing excess mortality and sudden deaths, the FLCCC doctors have made some suggestions based on their understanding of the processes that may be leading to the sudden cardiac events. They are, however, cautious because there has been no science or research effort put into understanding the causes of vaccine injury since major public health institutions continue to insist the vaccines are safe and effective and that side effects are rare and temporary.
“Knowing what we know of the science, of the consequences of these vaccines, and of the time distribution of these major events, we think it’s prudent to be on anti-platelets (aspirin) and fibrinolytics (nattokinase, lumbrokinase) in the hopes that somehow this mitigates or interrupts the development of these life-ending clots at five months out,” Dr. Kory advises.
Ideally, Dr. Marik says that asymptomatic patients who are in this time frame post-vaccination would be risk stratified, and those with moderate to high risk started on preventative measures. Unfortunately, since the risk of sudden death post-vaccine has not been generally recognized and has therefore not been studied, there is no data to allow for risk stratification.
In the absence of a risk-stratified approach, patients may wish to discuss the following interventions with a trusted healthcare provider:
- Daily low-dose aspirin (81 mg)
- Nattokinase (100-200 mg twice daily) (in those with low risk of bleeding)
- Omega-3 fatty acids (2-4 g daily)
- Resveratrol or flavonoid combination supplement
- Diet modulation (Low-carb, high-fat diet, low in omega-6 vegetable oils, avoiding processed foods)
In addition, since many deaths seem to occur during physical activity (think about the rash of sudden deaths in soccer players), vigorous physical activity (especially for younger people) should be avoided for at least 3 weeks following vaccination or boosting.
“Can we promise this will mitigate your risk? No. Do we think it’s going to save your life? No,” says Dr. Kory. “But these are potential protective interventions that are common sense, safe, pragmatic things you can do in the hopes of preventing such life-threatening events.”
To read more, see ‘An Approach to Managing Post-Vaccine Syndrome’.’https://covid19criticalcare.com/reducing-cardiac-risk-after-covid-19-vaccination/
‘Family Practice Physician, Dr. Bradley Meyers who founded the Okaboji Wellness Clinic after experiencing job loss for prescribing Ivermectin, talks about the disturbing censorship and pressure for doctors to follow CDC guidelines. Bradley also talks about patients that he was able to heal from Covid-19 through alternative methods to those recommended by the CDC.’https://rumble.com/v15sx21-family-physician-dr.-brad-meyers-talks-about-disturbing-pressures-and-censo.html?mref=6zof&mc=dgip3&ep=2
‘We know that SARS-CoV-2 is a man-made “paravirus” if you will, created in Wuhan/Moderna laboratories and reinforced by mainstream media propaganda. But in the grand scheme, at least the first iteration released onto the world, so-called COVID-19 is a lightweight illness that is mostly just rebranded influenza.
The mRNA and viral vector injections, along with Remdesivir, combine for a quick two-year, $200 billion global racket for big pharma and Bill Gates. Ivermectin is a proven, powerful drug to treat and prevent so-called COVID-19, according to 108 peer-reviewed studies. The Ivermectin Merck patents are long expired. So the cheap, $1-per-dose, Nobel Prize-winning drug poses a serious threat not only to the emergency use authorizations for the lethal injections, but also to the temporary COVID-19 racket. But those simply cannot be the only reasons for the persistent, petulant, childish mainstream media anti-Ivermectin propaganda.
The cancer industry will surpass $522 billion per year by 2028, according to Global Market Insights. Market analytics firm Precedent Research predicts the cancer industrial complex will surpass $581 billion annually by 2030. The COVID Blog™ has chronicled the strong correlation (perhaps causal relationship) between mRNA injections and cancer. Cancer has been a goldmine for big pharma since the 1960s. The average cancer patient is worth about $160,000 to the cancer industrial complex. Big pharma will never offer a cure, nor will the industry allow off-label, cheap, effective cancer treatments.
This blogger has seen scattered studies concluding that Ivermectin not only inhibits cancer cell growth, but also kills cancer cells. Perhaps placing nine said studies into one article can help disrupt the cancer industrial complex and wake up the snoozing masses.
1) American Journal of Cancer Research – 2018
This study by researchers at Unidad de Investigación Biomédica en Cáncer in Mexico concluded:
So far, at least 235 clinically-approved, non-cancer drugs have proven anti-tumor activity either in vitro, in vivo, or even clinically. Among these, ivermectin, an anti-parasitic compound of wide use in veterinary and human medicine, is clearly a strong candidate for repositioning, based on the fact that:
i) it is very safe, causing almost no side-effects other than those caused by the immune and inflammatory responses against the parasite in infected patients, and
ii) it has proven anti-tumor activity in pre-clinical studies. On the other hand, it is now evident that the use of very selective “unitargeted” drugs is commonly associated to early development of resistance by cancer cells, hence the use of “dirty” or “multitargeted” drugs is important to explore.
2) Pharmacological Research – 2020
Some key findings by Chinese researchers at Bengbu Medical College include the following:
- Recent studies have also found that Ivermectin (IVM) could promote the death of tumor cells by regulating the tumor micro-environment in breast cancer.
- In an experiment designed to screen potential drugs for the treatment of leukemia, IVM preferentially killed leukemia cells at low concentrations without affecting normal hematopoietic cells.
- In a study by Hashimoto, it found that IVM inhibited the proliferation of various ovarian cancer cell lines.
- Experiments confirmed that IVM could significantly inhibit the proliferation of five renal cell carcinoma cell lines without affecting the proliferation of normal kidney cells, and its mechanism may be related to the induction of mitochondrial dysfunction.
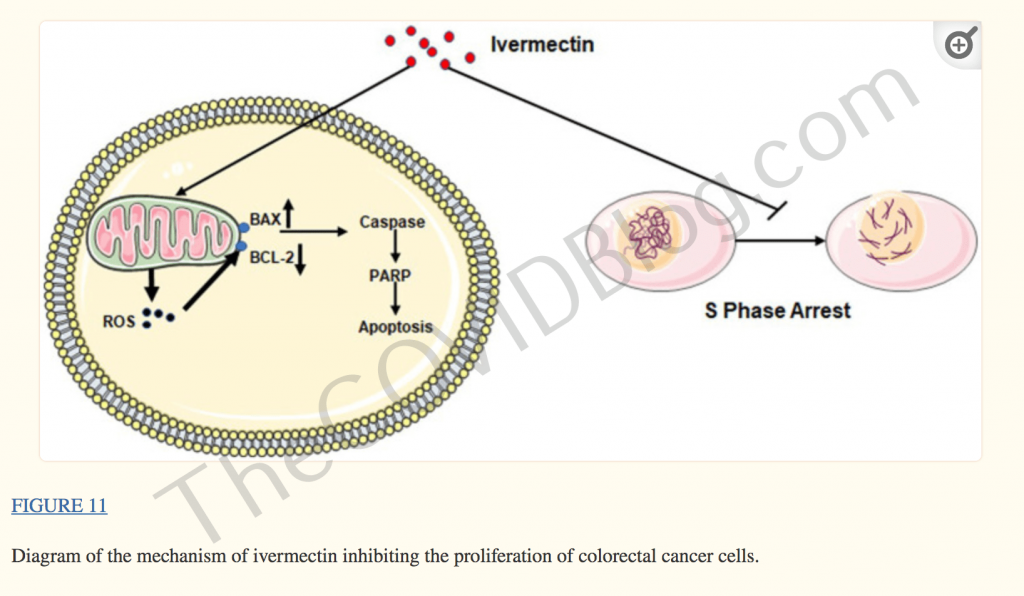
3) Frontiers in Pharmacology – 2021
Researchers at Henan University in China concluded:
We have demonstrated that ivermectin may regulate the expression of crucial molecules Caspase-3, Bax, Bcl-2, PARP, and Cleaved-PARP in the apoptosis pathway by increasing ROS production and inhibiting the cell cycle in the S phase to inhibit colorectal cancer cells (Figure 11). Therefore, current results indicate that ivermectin might be a new potential anticancer drug for treating human colorectal cancer and other cancers.
4) Molecular Medicine Reports – 2018
Researchers at the National Cancer Institute in Mexico City concluded the following:
Results from the present study demonstrated that ivermectin preferentially targeted the stem cell population in MDA–MB–231 human breast cancer cells. Ivermectin has been demonstrated to be safe, following treatment of millions of patients with onchocerciasis and other parasitic diseases, which makes it a strong candidate for further studies investigating its potential use as a repurposed drug for cancer therapy.
5) Biochemical and Biophysical Research Communications – 2017
Some key findings from researchers at The Second Clinical Medical College in China:
- Ivermectin is preferentially against renal cell carcinoma (RCC) while sparing normal kidney cells.
- RCC tumor growth in vivo is delayed by Ivermectin.
- Ivermectin induces mitochondrial dysfunction and oxidative stress.
- RCC has increased mitochondrial biogenesis than normal kidney cells.
6) EPMA Journal – 2020
Researchers at three Chinese institutions concluded:
Those findings provided the potential targeted lncRNA-EIF4A3-mRNA pathways of ivermectin in ovarian cancer, and constructed the effective prognostic model, which benefits discovery of novel mechanism of ivermectin to suppress ovarian cancer cells, and the ivermectin-related molecule-panel changes benefit for its personalized drug therapy and prognostic assessment towards its predictive, preventive, and personalized medicine (PPPM) in ovarian cancers.
7) BMC Cancer – 2021
Chinese researchers at Henan University, concluded the following:
We demonstrated that ivermectin effectively inhibit the proliferation of esophageal squamous cell carcinoma (ESCC) cells by inducing mitochondrial dysfunction, suppressing NF-κB signaling and promoting apoptosis. Our results suggest that ivermectin may be a potential therapeutic target against ESCC.
8) Cancer Chemotherapy and Pharmacology – 2020
Some key findings from researchers at Instituto Nacional de Cancerologia in Mexico City:
Ivermectin reduced both cell viability and colony formation capacity in the stem cell-enriched population as compared with the parental one. Finally, in tumor-bearing mice ivermectin successfully reduced both tumor size and weight. Our results on the anti-tumor effects of ivermectin support its clinical testing.
9) EMBO Molecular Medicine – 2014
Some key findings by University of Geneva researchers are as follows:
Constitutive activation of canonical WNT-TCF signaling is implicated in multiple diseases, including intestine and lung cancers, but there are no WNT-TCF antagonists in clinical use. We report that Ivermectin inhibits the expression of WNT-TCF targets, mimicking dnTCF, and that its low concentration effects are rescued by direct activation by TCFVP16.
In vivo, Ivermectin selectively inhibits TCF-dependent, but not TCF-independent, xenograft growth without obvious side effects. Given that Ivermectin is a safe anti-parasitic agent used by 200 million people against river blindness, our results suggest its additional use as a therapeutic WNT-TCF pathway response blocker to treat WNT-TCF-dependent diseases including multiple cancers.

